
Cranial Electrotherapy Stimulation
CES is an electromedical modality indicated for the treatment of anxiety and insomnia.
“Electrosleep treatment” – an older name for CES – came into the USA from Japan in the late 1960s. This therapy had been originally pioneered in Russia and other East Block countries. Since the current was directed across head, the FDA renamed it “Cranial Electrotherapy Stimulation (CES)” in 1978, and now allows its marketing in the USA for the treatment of anxiety and insomnia (CES regulatory status). A major use of CES has been in the treatment of symptoms of the drug abstinence syndrome, including severe anxiety, and insomnia. The medical use of CES is now becoming more widely indicated in the USA.
During a CES treatment, a mild electrical stimulus is applied transcranially with electrodes attached to the head. CES is a broad category and historically a variety of electrical devices have been used to perform this therapy. In most cases, however, the output has been limited to 1-2 mA of electrical stimulation. Modern CES devices use less than 1mA of low-frequency (0.5Hz) bi-phasic currents applied with the use of electrodes that attach to the patient’s ear lobes. An average length of treatment is generally 20-60 minutes. Daily treatments are recommended during the first 3-8 weeks of CES therapy.
Postulated mechanisms of Alpha-Stim® CES
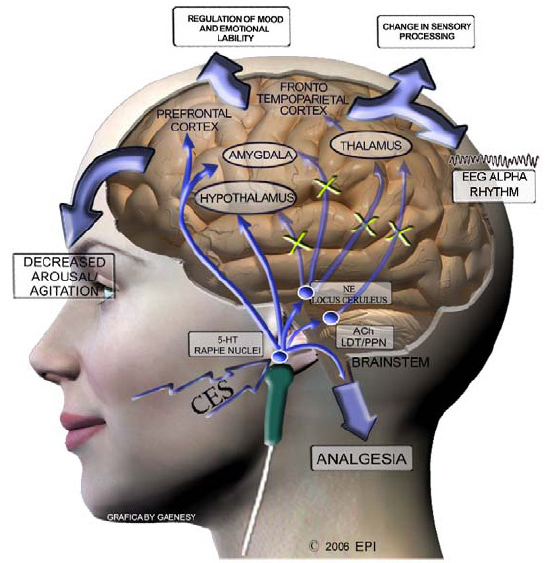
The exact mechanism by which Alpha-Stim® produces effects is not fully known. However, based on previous and ongoing studies, it appears that the Alpha-Stim® microcurrent waveform activates particular groups of nerve cells located at the brainstem, a site at the base of the brain that sits atop of the spinal cord. These groups of nerve cells produce the chemicals serotonin and acetylcholine, which can affect the chemical activity of nerve cells that are both nearby and at more distant sites in the nervous system. In fact, these cells are situated to control the activity of nerve pathways that run up into the brain and that course down into the spinal cord.
By changing the electrical and chemical activity of certain nerve cells in the brainstem, Alpha-Stim® appears to amplify activity in some neurological systems, and diminish activity in others. This neurological ‘fine tuning’ is called modulation, and occurs either as a result of, or together with the production of a certain type of electrical activity pattern in the brain known as an alpha state which can be measured on brain wave recordings (EEG). Such alpha rhythms are accompanied by feelings of calmness, relaxation and increased mental focus. The neurological mechanisms that are occurring during the alpha state appear to decrease stress-effects, reduce agitation and stabilize mood, and control both sensations and perceptions of particular types of pain.
These effects can be produced after a single treatment, and repeated treatments have been shown to increase the relative strength and duration of these effects. In some cases, effects have been stable and permanent, suggesting that the electrical and chemical changes evoked by Alpha-Stim® have led to a durable re-tuning back to normal function.
Neurological Modulation
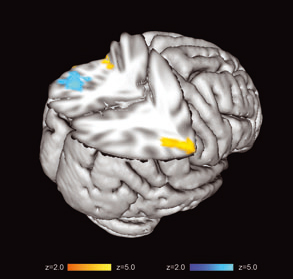
Cortical Brain Deactivation

Increase in Alpha Frequency Production
Cork et al. (2004). The effect of cranial electrotherapy stimulation (CES) on pain associated with fibromyalgia. The Internet Journal of Anesthesiology. Volume 8(2).
Lichtbroun et al. (2001). The treatment of fibromyalgia with cranial electrotherapy stimulation. Journal of Clinical Rheumatology, 7(2):72-78.
Brotman, P. (1989). Low-intensity transcranial electrostimulation improves the efficacy of thermal biofeedback and quieting reflex training in the treatment of classical migraine headache. American Journal of Electromedicine, 6(5):120-123.
Solomon et al. (1989). Safety and effectiveness of cranial electrotherapy in the treatment of tension headache. Headache. 29(7):445-50.
Capel et al. (2003). The amelioration of the suffering associated with spinal cord injury with subperception transcranial electrical stimulation. Spinal Cord. 41(2):109-17.
Tan et al. (2006). Using cranial electrotherapy stimulation to treat pain associated with spinal cord injury. Journal of Rehabilitation Research and Development, 43:461-474.
Alpher, E. J., and D. L. Kirsch (1998). Traumatic brain injury and full body reflex sympathetic dystrophy patient treated with cranial electrotherapy stimulation. American Journal of Pain Management, 8(4):124-128.
Kirsch, D. L. and R. B. Smith (2000b). The use of cranial electrotherapy stimulation in the management of chronic pain: a review. NeuroRehabilitation, 14(2):85-94.
Kirsch, Daniel L. (2002). The Science Behind Cranial Electrotherapy Stimulation, 2nd Edition, Medical Scope Publishing Corporation, Edmonton, Alberta, Canada, 224 pp.
James Giordano, Ph.D. (Center for Clinical Bioethics, Georgetown University Medical Center, Washington, DC).
Kennerly (2006). Changes in quantitative EEG and low resolution tomography following cranial electrotherapy stimulation. Ph.D. Dissertation, University of North Texas. 425 pp.